Showing posts with label childhood cancer. Show all posts
Showing posts with label childhood cancer. Show all posts
Monday, 6 June 2022
5 Types of Paediatric Cancer You Need to Know About
Here is another one I wrote a few years ago on the Max Healthcare platform. This talks about the 5 Types of Paediatric Cancer You Need to Know About
Sunday, 5 June 2022
Childhood cancer can be treated
I am in the process of bringing all y blog posts in one place. Here is something I wrote a few years ago on the Max Healthcare platform.
https://www.maxhealthcare.in/blogs/childhood-cancer-can-be-treated
It is intended for the general public. The types of cancer affecting children are quite different from the cancers that affect teenagers and young adults. Childhood cancers have become a menace. However, a lot of progress has been made in treating childhood cancers in the recent decades
Monday, 11 April 2022
SAFER Ukraine - The Power of the Global Pediatric Oncology Community
For the last few weeks, we have all watched with horror at the unfolding events in Ukraine. The casualties of war are not only the armed forces personnel, but also civilians (men, women and children) in Ukraine who have been caught in the cross-fire and the bombings of residential areas, theatres, markets and even hospitals.
According to https://en.wikipedia.org/wiki/2022_Ukrainian_refugee_crisis "More than 4.5 million refugees have since left Ukraine (as of 9 April 2022), while an estimated 6.5 million people have been displaced within the country (as of 18 March 2022). In total, more than ten million people – approximately one-quarter of the country's total population – had left their homes in Ukraine by 20 March. By 24 March 2022, according to UNICEF, more than half of all Ukrainian children had been forced to leave their homes."

SAFER Ukraine has established a virtual command center to coordinate evacuations and ensure treatment continues for pediatric oncology patients. The process includes determining transportation logistics and identifying high-risk patients who are deteriorating. The SAFER Ukraine team and volunteers translate medical records, coordinate departure travel and manage the logistics of transport across the border. In addition to the above efforts, the team also established a triage clinic in Poland. Patients and their families can rest and recover from the evacuation while awaiting assignment to a clinic for continued treatment.
According to https://en.wikipedia.org/wiki/2022_Ukrainian_refugee_crisis "More than 4.5 million refugees have since left Ukraine (as of 9 April 2022), while an estimated 6.5 million people have been displaced within the country (as of 18 March 2022). In total, more than ten million people – approximately one-quarter of the country's total population – had left their homes in Ukraine by 20 March. By 24 March 2022, according to UNICEF, more than half of all Ukrainian children had been forced to leave their homes."
Through these incredibly difficult times, there are many examples of individuals and groups which have come forward to the aid of the Ukrainian citizens. One such example is the SAFER UKRAINE initiative which stands for Supporting Action For Emergency Responses in UKRAINE and has been set up by St Jude Global along with multiple partners from the global pediatric oncology community including SIOP (International Society of Pediatric Oncology) and CCI (Childhood Cancer International).


SAFER Ukraine has established a virtual command center to coordinate evacuations and ensure treatment continues for pediatric oncology patients. The process includes determining transportation logistics and identifying high-risk patients who are deteriorating. The SAFER Ukraine team and volunteers translate medical records, coordinate departure travel and manage the logistics of transport across the border. In addition to the above efforts, the team also established a triage clinic in Poland. Patients and their families can rest and recover from the evacuation while awaiting assignment to a clinic for continued treatment.
Through these efforts, more than 800 Ukrainian children with cancer have been registered and over 500 have been transferred to clinics in Poland, Germany, Italy, Netherlands, France, Spain, United Kingdom, Czech Republic, Austria, Switzerland, Canada and USA. In my 15 years of experience of engaging with the global pediatric oncology community (which has always been sensitive to healthcare disparities and has continually worked to improve the outcomes of those in resource-limited settings) such a concerted advocacy and humanitarian effort is unprecedented and I can only applaud and wish them well.
Tuesday, 15 March 2022
Dinutuximab (Anti GD2 therapy) for children with high risk neuroblastoma now available in India
High risk neuroblastoma continues to be a childhood cancer which is challenging to treat and has poor outcomes. While smaller increments in survival have been made over the years, a big step-up in survival was when Anti-GD2 therapy (now known as Dinutuximab) was introduced and this was published by Yu et al in this landmark study. I had written a blog on this in 2010 and also reflected on the Indian situation. Since then Dinutuximab has become the standard of care for high risk neuroblastoma in high-income countries.
Low and middle income countries like India have not had access to the medicine, either through clinical trials, or through compassionate use. This has now changed and the first child received Dinutuximab in Mumbai last year and this was covered in the media - Mumbai child receives special injection to treat rare cancer. Subsequent to this, I have been informed that another child has received this treatment in Bangalore and there are a few others waiting to receive it.
While this is exciting and welcome, it is important to point out that AVAILABILITY does not equate to ACCESSIBILITY. And the main reason for that in this context is AFFORDABILITY. This drug is not manufactured in India but imported from Europe. Based on the information available to me, a child who weighs around 13 kg will need 3 vials per cycle and a total of 15 vials for 5 cycles. With each vial 11,000 Euros, the total cost is approximately INR 1.4 cr + 25% custom duties. With the right kind of paper-work and eligibility for discount, the custom fees may be waived off and the price of the drug could come down to INR 56 lakh. But this still remains out of reach of almost all children with high risk neuroblastoma in India.
In conclusion, it is a welcome positive step that Dinutuximab in now available in India. With time and increased use, we hope and expect the price to be driven down so that it becomes accessible to more children who need it.
Monday, 28 February 2022
A Parents Guide to Childhood Cancer - The Max Institute of Cancer Care Version
When a child is diagnosed with cancer, the family faces a variety of new medical terms and challenges. It is vital that parents understand the many aspects of the illness and treatment, as well as the experiences they may face and have to cope with during the treatment process. At such times, consistent, repeated and reliable information is invaluable. One way to deliver this is through written information in simple language targeted at parents and carers. There are many resources available online - here are two of my favourite ones - The Children's Oncology Group Family Handbook and the Children's Cancer and Leukemia Group Parents Guide.

I had not been able to find a similar good resource targeted at parents of children with cancer in India till I came across and excellent resource made by St Jude India ChildCare Centres and the clinical team at Tata Memorial Centre, Mumbai. With their permission we have now adapted for the use of our parents whose children are being treated at Max Institute of Cancer Care. They are available in English and in Hindi.
Thursday, 15 October 2020
Milestones in Childhood Cancer Collaborative Research - Part 2
The 21st century has see the emergence of multi-centre collaborative research from low and middle income countries with reports from Central America, Africa, China and India. This is a very welcome development and I will briefly describe some of these initiatives below. But I would like to start with Brazil where cooperative groups for childhood cancer started in the 1980s.
The Brazilian Experience
The Cooperative Groups Initiative in Brazil started in 1980, allowing exchange of expertise and proposals of better care. There are seven well-established cooperative groups with ongoing protocols including the participation in international studies. Among their earliest works which was published in 1991 was the randomised controlled study on Single‐dose versus fractionated‐dose dactinomycin in the treatment of wilms' tumor with no significant difference in overall or relapse‐free survival. Shortly afterwards, they published the Treatment results of three consecutive Brazilian cooperative childhood ALL protocols: GBTLI-80, GBTLI-82 and -85 and were able to examine the role and dose of cranial radiation as well as treatment intensification.
For further reading - Brazilian Society of Pediatric Oncology - SOBOPE: 30 years of history, a lot in the present, full of the future and Pediatric hematology oncology in Brazil
Francophone Africa - The French‐African Pediatric Oncology Group (GFAOP)

The Franco-African Childhood Cancer Group (French acronym, GFAOP) was founded in 2000 with aim of improving the outcomes of children with cancer in Africa. The GFAOP has developed two forms of action. The main form consists of organizing two- to twelve-month training sessions for physicians and nurses in France and Morocco. The other form involves assessing the feasibility of modern treatment protocols for various cancers in Africa. The first feasibility trials were carried out on nephroblastoma and Burkitt's lymphoma in 12 pilot units in North Africa, West Africa, and Madagascar. In the first study from 2001 to 2004, 306 children of Burkitt's lymphoma using French LMB protocols adapted to the African setting and achieved a survival rate of 61% - Treatment of B‐cell lymphoma with LMB modified protocols in Africa—report of the French‐African Pediatric Oncology Group (GFAOP).
For further reading (In French) - Treatment of childhood cancer in Africa. Action of the Franco-African childhood cancer group
The SIOP PODC Africa Wilms Tumour Project
This project is implementing a SIOP PODC adapted treatment guideline for Wilms tumour in several centres in sub-Saharan Africa. This is done as a multi centre prospective clinical trial with uniform outcome evaluation. The project started in 2014. More than 300 patients have been included and treated. End of treatment survival without evidence of disease increased from 52% to 68%. Death during treatment decreased from 21% to 13% and abandonment of treatment from 23% to 13% - Improved outcome at end of treatment in the collaborative Wilms tumour Africa project

Asociación de Hemato‐Oncologiá Pediátrica de Centro América (AHOPCA)
Inspired by the twinning program of Manuel de Jesus La Mascota Hospital in Managua, Nicaragua and the Pediatric Clinic of the University of Milano‐Bicocca in Monza, Italy as well as the subsequent establishment of the Monza International School of Pediatric Hematology‐Oncology (MISPHO), the Asociación de Hemato‐Oncologiá Pediátrica de Centro América (AHOPCA) was formed in 1998. Initially this consisted of Guatemala, Honduras, El Salvador, Nicaragua, and Costa Rica. Panama joined in 2001 and the Dominican Republic in 2006

Their early collaborative research works have been in the area of Nutrition and Retinoblastoma.
For further reading - Asociación de Hemato-Oncología Pediátrica de Centro América (AHOPCA): a model for sustainable development in pediatric oncology
There are several other regional and national initiatives in pediatric oncology collaborative research in LMIC which have blossomed in recent years e.g. the Turkish Pediatric Oncology Group, The Pediatric Oncology East and Mediterranean (POEM) network and others. We look forward to seeing their work in the future. I would like to now focus on China and India, which together would constitute nearly a third of the childhood cancer burden. And so both of these countries have to strengthen their collaborative research so that they individually and the world collectively can aspire to reach the WHO Global Initiative for Childhood Cancer target of at least 60% survival by 2030.
The Chinese Experience
There are two national collaborative groups within China. The Chinese Children Leukemia Group (CCLG) started the CCLG-ALL 2008 Study. A total of 2231 patients were recruited from 10 hospitals across the country from 2008 to 2013 - Outcome of children with newly diagnosed acute lymphoblastic leukemia treated with CCLG-ALL 2008: The first nation-wide prospective multicenter study in China. More recently, the Chinese Children Cancer Group (CCCG) which was formed in In 1997 under the China Anti-Cancer Association, has organized one of the largest clinical trials in China, the CCCG-ALL-2015 Study. The study is led by the National Center for Children’s Health (Shanghai) and supported by St Jude Children’s Research Hospital and the VIVA Foundation. Up to January 2019, and 6024 patients were recruited into the study.
For further reading - Treatment of childhood cancer in China: Current status and future direction
Indian Pediatric Oncology Group (InPOG)
The earliest report of collaboration in the field of pediatric oncology in India was that between Cancer Institute, Chennai and the National Cancer Institute, USA in the early 1980s. Adopting a more intense protocol (MCP841) than that being used at the time, led to an improvement in the event free survival of acute lymphoblastic leukemia from 20% to 40%. This treatment strategy was then adopted by Tata Memorial Hospital, Mumbai in 1986 and All India Institute of Medical Sciences, New Delhi in 1992. With this common protocol, event free survival rates of 40-60% were achieved - Treatment of acute lymphoblastic leukaemia in countries with limited resources; lessons from use of a single protocol in India over a twenty year period.
The need to establish a national cooperative group in order to develop prospective multi-centre clinical trials in India became increasingly apparent. Such a strategy was critical to understand the biological differences in the disease, to assess responses to treatment and ultimately to improve childhood cancer survival in India. Active since 2015, the mission of InPOG is to improve the outcomes of children with cancer in India by collaborative research. At present here are 26 disease and discipline subcommittees with a portfolio of 31 studies.
The InPOG-HL-15-01 was amongst the first studies to start recruitment and standardised therapy of children with Hodgkin disease on an ABVD backbone – InPOG-HL-15-01 - Challenges and lessons learnt in setting up the first collaborative multicentre prospective clinical trial in childhood cancer in India. Initial results are expected to be published next year.
For further reading - Indian Pediatric Oncology Group (InPOG) - Collaborative research in India comes of age
The future looks very exciting. May this momentum gather an even greater speed!
Wednesday, 16 September 2020
Milestones in Childhood Cancer Collaborative Research - Part 1
September is Childhood Cancer Awareness Month and it is a good time to reflect on the progress we have made in curing childhood cancer and how we got here. An important part has been the ability of all stakeholders to get together and enroll children with cancer on to clinical trails, specially multicentre collaborative research. In this first part I look at some of the earliest works done in North America and Europe and highlight a few studies.

This all started in 1948 when Sidney Farber attempted to use a folate antagonist, Aminopterin to block the function of folic acid in patients with acute leukemia in hopes of achieving remission - Temporary remissions in acute leukemia in children produced by folic acid antagonist, 4-aminopteroyl-glutamic acid. Of 16 children, 10 demonstrated clinical, hematological and pathological evidence of improvement for three months. At that time this observation was met with disbelief and also it was felt to be unethical to "experiment" with the life of a child with leukemia when cure was not possible.
Thankfully, he and others like him continued in their efforts. The relative rarity of the disease and the need for shared expertise in management led to the creation of the first pediatric oncology co-perative groups (Cancer and Leukemia Group B Cooperative Group as well as the Acute leukemia Chemotherapy Cooperative Study Group A) in the US in 1955 which were the forerunners of the now well established and respected Children's Oncology Group. For the last 65 years, COG in North America and SIOP in Europe have increased our knowledge and understanding of childhood cancers and conducted studies which have improved outcomes. Here are some of the earliest studies:
Childhood Leukemia
Published by Heyn et al in 1960, The Comparison of 6-Mercaptopurine with the Combination of 6-Mercaptopurine and Azaserine in the Treatment of Acute Leukemia in Children: Results of a Cooperative Study was the first multi-centre co-operative clinical trial in childhood cancer. In 125 cases of previously untreated acute leukemia in children, no significant difference was seen in the percentage of complete remissions obtained when 6-mercaptopurine was used alone or when 6-mercaptopurine and azaserine were used in combination. The median duration of the complete remissions for the combination therapy was 4.12 months compared to 2.75 months for 6-mercaptopurine alone and the difference was not statistically significant.
At the same time, Freireich et al studied 6-Azauracil in patients with "advanced" acute leukemia, refractory to standard chemotherapy - Evaluation of a New Chemotherapeutic Agent in Patients with "Advanced Refractory" Acute Leukemia. Studies of 6-Azauracil. Under the conditions of the study this compound was found to have no significant antileukemic activity.
Two decades later, in 1980, the first collaborative efforts in childhood ALL from Europe were published on children treated on the BFM 70/76 protocol - The Berlin Childhood Acute Lymphoblastic Leukemia Therapy Study, 1970–1976. The treatment protocol consisted of vincristine, prednisone, daunorubicin, L-asparaginase, cyclophosphamide, cytarabin, 6-mercaptopurine, intrathecal methotrexate, and cranial or craniospinal irradiation. Maintenance therapy was cyclic sequential administration of intravenous methotrexate and oral 6-mercaptopurine with 6-week reinduction pulses of prednisone/vincristine. 56.2% of patients were in complete continuous remission for a median of 67 months.
Childhood Solid Tumours
Following the work on childhood leukemia, cooperative groups simultaneously also started looking at solid cancers. Earliest work was done on Wilms tumour on both sides of the Atlantic.
Published in 1968, maintenance dactinomycin following surgery was found to be superior (continued remission rate of 86%) compared to when no maintenance was given (continued remission rate of 48%) - Single versus multiple dose dactinomycin therapy of Wilms's tumor. A controlled co-operative study conducted by the Children's Cancer Study Group A (formerly Acute Leukemia Co-operative Chemotherapy Group A)
Colleagues in Europe investigated the role of radiotherapy and actinomycin d (dactinomycin) in Wilms tumour - Preoperative versus postoperative radiotherapy, single versus multiple courses of actinomycin d, in the treatment of Wilms' tumor. Preliminary results of a controlled clinical trial conducted by the international society of paediatric oncology (S.I.O.P.). This was the first SIOP study and also the first international randomized trial in Europe. Pre-op radiotherapy reduced the tumour rupture rate at surgery. Also there was no added benefit of post-op radiotherapy after receiving pre-op radiotherapy.
Published in 1968, maintenance dactinomycin following surgery was found to be superior (continued remission rate of 86%) compared to when no maintenance was given (continued remission rate of 48%) - Single versus multiple dose dactinomycin therapy of Wilms's tumor. A controlled co-operative study conducted by the Children's Cancer Study Group A (formerly Acute Leukemia Co-operative Chemotherapy Group A)
Colleagues in Europe investigated the role of radiotherapy and actinomycin d (dactinomycin) in Wilms tumour - Preoperative versus postoperative radiotherapy, single versus multiple courses of actinomycin d, in the treatment of Wilms' tumor. Preliminary results of a controlled clinical trial conducted by the international society of paediatric oncology (S.I.O.P.). This was the first SIOP study and also the first international randomized trial in Europe. Pre-op radiotherapy reduced the tumour rupture rate at surgery. Also there was no added benefit of post-op radiotherapy after receiving pre-op radiotherapy.
Childhood CNS Tumours
It was in 1990, that the first multicentre co-operative group studies were published on childhood CNS tumours in North America and Europe, almost at the same time. Both looked at the role of adjuvant chemotherapy in medulloblastoma.
Evans et al from the Children's Cancer study Group (another forerunner of COG) studied the benefit of adjuvant vincristine, CCNU and prednisolone after surgery and radiation in children with medulloblastoma - The treatment of medulloblastoma - Results of a prospective randomized trial of radiation therapy with and without CCNU, vincristine, and prednisone. It is concluded that chemotherapy does not benefit patients with low-stage medulloblastoma, but may benefit those with more advanced stages of disease.
Tait et al from SIOP examined adjuvant vincristine and CCNU in medulloblastoma - Adjuvant chemotherapy for medulloblastoma: The first multi-centre control trial of the International Society of Paediatric Oncology (SIOP I). Their results were that although there was no overall statistical difference between the two arms of the trial, a benefit for chemotherapy was seen in a number of sub-groups; partial or sub-total surgery, brainstem involvement , and stage T3 and T4 disease.
Tait et al from SIOP examined adjuvant vincristine and CCNU in medulloblastoma - Adjuvant chemotherapy for medulloblastoma: The first multi-centre control trial of the International Society of Paediatric Oncology (SIOP I). Their results were that although there was no overall statistical difference between the two arms of the trial, a benefit for chemotherapy was seen in a number of sub-groups; partial or sub-total surgery, brainstem involvement , and stage T3 and T4 disease.
Childhood Cancer Survivors
By the end of the 20th century collaborative research in childhood cancer survivors was in flow and the first publication from the Childhood Cancer Survivor Study came out. Marriage in the survivors of childhood cancer: A preliminary description from the childhood cancer survivor study showed a decreased likelihood of marriage among childhood cancer survivors, which may be influenced by gender and/or race
These studies are only a tiny reflection of the huge amount of collaborative work and scientific output which took place in the second half of the 20th century. Noticeably, there was a complete absence of such work from low and middle income countries (LMIC). Health professionals in these settings were also working hard to provide the best possible care to their patients while being hampered by limited resources. They were however unable to translate their efforts into regional or national collaborative efforts. Progress in this area happened much later and in my next blog post I will showcase milestones of childhood cancer collaborative research in LMIC.
Tuesday, 1 September 2020
Childhood Cancer Awareness Month: increasing survival rates for children with cancer
From UICC
1 September 2020
Saturday, 15 August 2020
Cancer and Childhood Cancer Care in India – FIVE reasons why I am POSITIVE and MOTIVATED on our 74th Independence day

Today we complete 73 years of our independent existence and celebrate our 74th Independence day. The strides we have made as a nation are truly enormous and are acknowledged widely. At the same time, the challenges which remain are no less mighty and we need to continue on the path of relentless progress to overcome hunger, poverty, ill health, strife, pollution, among others.
At this
time I reflect on the cancer and childhood cancer care in India, and despite
the many challenges which we face in this area, I have found FIVE reasons why I
as a pediatric oncologist am POSITIVE and MOTIVATED on this day and look forward
to the coming year and decade with great anticipation.
REASON ONE –
WHO Global Initiative for Childhood Cancer (GICC)
Active
involvement of the WHO and launch of the GICC in 2018 (https://www.who.int/cancer/childhood-cancer/en/) has been a landmark development for all stakeholders in pediatric oncology
across the world. Work has already started in several countries including
Myanmar which is in the South Asian region. Some work has also begun in India
last year with meetings with the professional societies and the parent groups.
This year, the Ministry of Health and Family Welfare, Government of India along
with the WHO SEARO office have selected 4 centres (BBCI Guwahati, Kidwai
Hospital Bangalore, Kalawati Saran Hospital New Delhi and Tata Memorial
Hospital Mumbai) to be National Centres of Excellence for Childhood Cancer
services. Many more activities and initiatives will follow to help India reach
the target of 60% survival rate for children with cancer by 2030.
REASON TWO –
National Cancer Grid (NCG)
For too
long we have had a plethora of national societies in all spheres of medicine
including oncology and pediatrics, which seem to exist from meeting to meeting,
seminar to seminar. Most professional medical societies in India have not taken
up the cause of the patient, and addressed the deficiencies in healthcare in a big
way. Enter National Cancer Grid (https://tmc.gov.in/ncg/) in 2012 – today it is a network of >200
major cancer centers, research institutes, patient groups and charitable
institutions across India. Led very ably by Dr CS Pramesh it has launched and
successfully executed a host of collaborative activities – Disease Management
Group specific Virtual Tumour Boards, Online second opinion service through
Navya, CRedO Workshop for researchers, are just a few of the many initiatives which
are ongoing or in development.
REASON
THREE – Indian Pediatric Oncology Group (InPOG)
Multicentre
collaborative research is critical if India wants to make progress in the care
and outcomes of its children with cancer. InPOG (https://www.phoindia.org/cms/inpog-faqs) has been active since the
beginning of 2015 and as of December 2019 (in five years) 5543 patients have
been recruited in 15 studies (40% interventional and 60% non-interventional
studies) from 90 centres. It now enters into its next phase and promises faster and greater developments.
REASON
FOUR – Cankids
Driven
by the relentless energy of its founder Poonam Bagai, Cankids (https://www.cankidsindia.org/) has blazed the trail
in India as well as globally, showcasing how patients, parents and civil
society can contribute to childhood cancer care. They not only provide vital
social and psychological support for children with cancer and their families,
but are leading engagement with state governments on Change for Childhood
Cancer in India (http://childhoodcancerindia.blogspot.com/2017/09/supporting-childhood-cancer-treatment.html)
and have done a phenomenal amount of work during COVID-19 ensuring that the
treatment of patients is not disrupted.
REASON
FIVE – Max Healthcare and Max Institute of Cancer Care
My workplace
and my employer (https://www.maxhealthcare.in/) have consistently demonstrated, never more than now in these
COVID-19 times, that it is possible to deliver high quality care to cancer
patients while balancing social responsibility and driving academics and
research in the private sector. Solving India’s healthcare challenges would
need partners in all sectors of healthcare and Max has shown the way. Thank you
Mr Abhay Soi and Dr Harit Chaturvedi for your inspirational leadership
Thursday, 30 July 2020
Childhood cancer survivorship and late effects: The landscape in India in 2020
Cure from childhood cancer is now a justifies expectation and with the right treatment most children would get cured of their cancer and achieve long-term survival. While the goal is that this long-term survival is normal, experience has taught us that some survivors suffer from late side-effects. This has been an area of intense focus in the last few decades and there is now growing evidence on how to prevent and treat these late side-effect.
So far, the information from India has been limited and scattered. We mad an attempt to bring this all together and are happy to share our recent publication on this in the Pediatric Blood Cancer - Childhood cancer survivorship and late effects: The landscape in India in 2020
We highlight not only the steadily increasing work going on with childhood cancer survivors in the hospitals, but also the efforts taken by healthcare providers, and other stakeholders in developing this service, advocating for this cause and providing survivors with a platform. A special mention of two such organisations - Ugam and Cankids - who contributed to this effort.
Sunday, 19 July 2020
COVID-19 Pandemic and Childhood Cancer
None of us has ever seen anything like this before. And I am not talking about a viral infection. I am talking about the emergence of a new infection and the global and national response to it which has been without parallel. Over the last few months not only has the infection affected the health of millions and taken the lives of hundreds of thousands, it has brought the world to a HALT! Individuals, businesses and countries have borne the brunt of it and continue to do so.
It will be some time before this comes to pass. Meanwhile children with cancer (like those with many other illnesses) have been caught in this maelstrom with impact on their diagnosis, their treatment and eventually outcomes. In the face of such ongoing challenges, the global and the national pediatric oncology community has got together to respond on multiple fronts in many different ways.

The Global COVID-19 Observatory and Resource Center for Childhood Cancer is one such effort. Developed by SIOP and St Jude Global, this Resource Centre provides all relevant information to those caring for children with cancer including parents and families. The reader is encouraged to browse the website for further information.
It will be some time before this comes to pass. Meanwhile children with cancer (like those with many other illnesses) have been caught in this maelstrom with impact on their diagnosis, their treatment and eventually outcomes. In the face of such ongoing challenges, the global and the national pediatric oncology community has got together to respond on multiple fronts in many different ways.

Specifically I wanted to highlight two things.
Firstly, are the weekly COVID Conversations - a live webinar to discuss difficult issues, address pressing questions, and hear the experiences of our colleagues when it comes to caring for children with cancer during this pandemic. Several such Conversations have happened with one specifically relating to Experiences in India and Pakistan.
Secondly, is the Global Registry of COVID-19 in Pediatric Cancer which provides a visualisation of the impact of the virus on our patient population.
Tuesday, 10 March 2020
Podcast on perspectives of caregivers of children with cancer in India on their journey to accessing timely cancer diagnosis and treatment

I am glad to share a podcast https://www.ghccpod.com/22-the-labyrinth/ was conducted by Dr Mark Zobeck based on one our recent pieces of work in trying to understand the experiences of the caregivers of children with cancer in India as they obtain their diagnosis and start treatment.
I quote from his link
How does a child with cancer in India access care?
If you’ve ever had an illness that was difficult to diagnose, you know that navigating the medical system can be incredibly frustrating. Bouncing back and forth between doctors, taking time off of work or school, waiting for hours upon hours, all while you don’t feel well and do not know what is going on with your body is enough to drive anyone crazy. Unfortunately for families of children with cancer, they know this feeling all too well. Childhood cancer can be very difficult to diagnose and the journeys that families undergo to find answers and receive care can be long and grueling.
To better understand these journeys, Drs. Neha Faruqui, Ramandeep Arora, and their colleagues have studied what they call the “healthcare labyrinth” of accessing childhood cancer care in India. Through discussions with parents and caregivers, they classified the major themes that contribute to difficult or prolonged paths to care. Today on the podcast, we will discuss their findings from their many hours of listening to the families’ stories.
I would encourage anyone listening to the podcast to also read their paper. As I say in the podcast, it reads more like a novel than a journal article, and I found myself emotionally invested in the way the parents described their journeys. It made me appreciate anew how important it is to establish robust health systems that can rapidly identify patients and refer them to appropriate tertiary care.
Lastly, this discussion is not meant to be a criticism of the Indian healthcare system. It is an enormous system that is responsible for caring for 1.3 billion people! There are many things it does very well! But of course, there are things that can be improved. As Dr. Arora says in the episode, this paper, and our discussion is about listening to the caretakers to discover how providers everywhere can better care for not only the patient during treatment but for the entire family through the entire cancer experience.
Read the full study here: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-019-7911-x
Sunday, 16 February 2020







Sunday, 18 February 2018
International Childhood Cancer Day 2018

15th Feb is celebrated as International Childhood Cancer Day every year across the world. This day celebrates those who have successfully conquered this disease and remembers those who did not make it. It spotlights the problem and the solutions. It brings together all stakeholders who are fighting to address this problem.

On this occasion several international and national organisations take a renewed pledge of commitment to these patients. Below are two press releases - the first by SIOP and CCI and the second by Cankids
Together for Advancing Cures, Transforming Care, Instilling Hope
Childhood Cancer International and SIOP are not alone in recognizing the devastating impact of childhood cancer on children and families around the globe. In September 2011, the United Nations (UN) General Assembly issued a Political Declaration recognizing four major Non-Communicable Diseases/NCDs (cancer, cardiovascular disease, diabetes and chronic respiratory disease) as the greatest killers of adults and children.
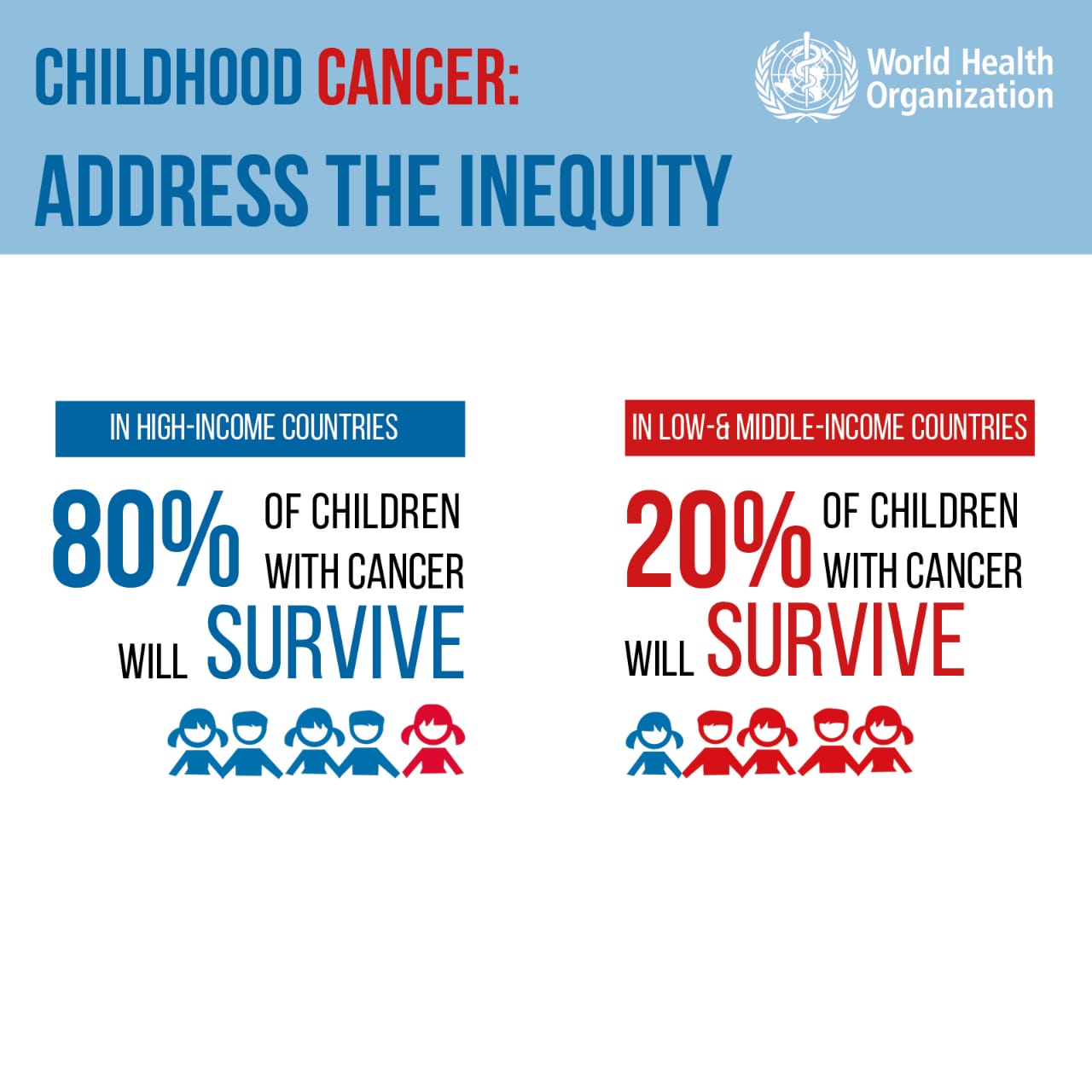
Sadly, childhood cancer continues to be the leading cause of non-communicable related death in children throughout the world. Globally, more than 300,000 children are diagnosed with cancer each year. Approximately 80 percent of our world’s children with cancer live in low-middle-income countries (LMICs) where more than 80 percent of these children die of their disease. In developed countries like the United States, Canada, United Kingdom, Japan and others, more than 80 percent of children survive cancer with hope to live productive and meaningful lives.
On December 13, 2017 a new report from WHO and the World bank revealed that approximately half of the world’s population, including children, do not have access to essential health services and that 800 million people spend at minimum 10 percent of their household income on health-related care. Childhood cancers are often curable but too many children and adolescents have no hope to overcome their disease simply because they were born in a country entrenched in poverty resulting in late diagnosis, lack of access to life-saving essential medicines and appropriate treatment. As childhood cancer organizations, we know only too well that the associated cost to treat a child with cancer can be a burden that too many families simply can’t overcome. We support the need for universal access to essential medicines and healthcare for all children in the world diagnosed with cancer. In order for this to happen, CCI and SIOP agree that making childhood cancer a national and global child health priority is a critical first step towards increasing access to treatment and reducing childhood cancer mortality.
All children in the world deserve hope for a cure - no matter where they live - not more excuses. We can no longer sweep this issue “under the rug.” Children are the future of our country and our world. Their vitality is the heartbeat of our world, a shared passion that can unite us because our future as a global community depends on it.
On International Childhood Cancer Day, all members of Childhood Cancer International and SIOP stand united to make childhood cancer a national and global child health priority to ensure there are adequate resources to meet the basic rights of children with cancer. We believe those basic rights for all children diagnosed with cancer include:
- The right to early and proper diagnosis;
- The right to access life-saving essential medicines;
- The right to appropriate and quality medical treatments, and;
- The right to have access to sufficient palliative care;
- The right to follow up care, services and sustainable livelihood opportunities for survivors.
RAISE YOUR VOICE TOGETHER WITH CHILDREN WITH CANCER
I DESERVE – MY CHILDHOOD MY LIFE
New Delhi 15th February 2018
February 15th is celebrated worldwide as International Childhood Cancer Day – aimed at creating awareness and advocating for childhood cancer as much for honoring the bravery and courage of children fighting cancer in our State, country and worldwide.
Internationally Childhood Cancer Day is spearheaded by Childhood Cancer International – an umbrella organization of 188 parent, survivor and social support organizations like Cankids, in collaboration with SIOP (International Society of Pediatric Oncologists). http://www.cankidsindia.org/iccd-2018.html)
Every year Cankids Kidscan, National Society for Change for Childhood Cancer, and member of Childhood Cancer International (CCI) celebrates ICCD across the country. Last year, 1580 children with cancer from 21 cities across India attended the ICCD celebrations. Children at all centers visited a monument of the city to celebrate ICCD and teachers educated children about the monument and how it symbolizes victory in some battle. The “We Are One” Childhood Cancer solidarity song was translated into regional languages and sung by children in different cities.
This February 15th, 2018 happy to inform you that this year we are doing it in a much bigger and grander way together with many other NGO partners and childhood cancer treating centers.
Our theme for ICCD is Go Gold India – Mera Haq, Mera Bachpan, Mera Jeevan – I Deserve My Childhood My Life. Families will participate in “I Deserve competitions and we will have kite making activities at the Learning activity Clinics in OPD and Wards, where children will make kites and together with their families write their prayers and messages. Children will be taken for an outing to a park where they can fly kites. The messages on the kite will reflect our theme and advocate to the governments that “Childhood Cancer should be a Child Health Priority in India”. We will be celebrating ICCD at all our 51 centers as well as those of our partners, across India.
Childhood Cancer is the low hanging fruit for a country’s cancer control program. In 2015 Cankids…KidsCan Launched The Go Gold India- Survivor Led Advocacy Campaign with 8 demands – To make Childhood Cancer Child Health Priority in India- a clear childhood cancer control plan and policy, more and dedicated pediatric oncology cancer centers, better and qualified manpower and health professionals, affordable but quality treatment and drugs, focused interventions for specific childhood cancers that are highly curable like Hodgkins Lymphoma, Retinoblastoma (eye cancer) and Wilms Tumor (kidney cancer), acceptance of the age of childhood cancer upto 18 years of age, and family and civil society engagement.
Sunday, 17 September 2017
Supporting Childhood Cancer Treatment in Punjab - Government of Punjab joins other Stakeholders
Childhood cancer almost never figures on the government radar. And we all realize that this is a critical component if we have to have real success in true control of childhood cancers in India. Individuals and organisations – where from the healthcare sector or the non-governmental sector can only do so much.
Over the last couple of years, Cankids has been actively engaging and lobbying with state governments – of Tamil Nadu and then Uttar Pradesh. Earlier this week they had a very fruitful meeting with the Punjab Government. I am sharing some news stories with you in this regard.
http://www.hindustantimes.com/punjab/cashless-cancer-treatment-for-all-below-18-punjab-health-minister/story-YeYJtKKcAbV584lwOqqneK.html
http://www.babushahi.com/full-news.php?id=63475&headline=Cashless-Cancer-treatment-for-children-at-18-empanelled-Punjab-hospitals
The Punjab government represented by the Punjab health minister Brahm Mohindra and his team joined the medical community – Dr Shruti Kakkar from DMC Ludhiana, Dr Joseph John from CMC Ludhiana, Dr Amita Mahajan from Apollo, New Delhi as well as Dr Scott Howard from World Child Cancer and International Society of Pediatric Oncology. The parent/patient support groups and civil society was represented by Cankids.
At a open meeting hosted at Government Medical College Patiala, several announcements were made including
Over the last couple of years, Cankids has been actively engaging and lobbying with state governments – of Tamil Nadu and then Uttar Pradesh. Earlier this week they had a very fruitful meeting with the Punjab Government. I am sharing some news stories with you in this regard.
http://www.hindustantimes.com/punjab/cashless-cancer-treatment-for-all-below-18-punjab-health-minister/story-YeYJtKKcAbV584lwOqqneK.html
http://www.babushahi.com/full-news.php?id=63475&headline=Cashless-Cancer-treatment-for-children-at-18-empanelled-Punjab-hospitals
The Punjab government represented by the Punjab health minister Brahm Mohindra and his team joined the medical community – Dr Shruti Kakkar from DMC Ludhiana, Dr Joseph John from CMC Ludhiana, Dr Amita Mahajan from Apollo, New Delhi as well as Dr Scott Howard from World Child Cancer and International Society of Pediatric Oncology. The parent/patient support groups and civil society was represented by Cankids.
At a open meeting hosted at Government Medical College Patiala, several announcements were made including
- Extend cashless cancer treatment for the children at the 18 empanelled hospitals
- To provide tertiary health services to each and every child of state suffering from cancer
- commenced first of its kind ever special awareness programme for children suffering from cancer
- Under the Chief Minister Cancer Relief Fund scheme, cancer patients will be given Rs 1.5 lakh for treatment
- The health department is also imparting special training to medical officers, staff nurses and auxillary nursing midwives (ANMs) to conduct tests concerning cancers, especially among children and women in rural areas
Of course, this is but the first step. Continued action will lead to change and that remains to be seen.
Wednesday, 26 July 2017
Childhood cancer in India and abandonment of treatment
I have often touched upon the phenomenon of abandonment of treatment in this blog. This happens when a child either does not start treatment or does not complete treatment. If this happens, then the child is likely not to get cured of their cancer. One may ask, why would a print not get their child treated appropriately. But this is the reality. Abandonment of treatment is the culmination of many inter-related factors.
Recently a journalist Ankur Paliwal contacted me as he wanted to highlight this issue. He met others as well and has published a nice piece which tries to bring together all viewpoints and highlights very well, the social problem that abandonment of treatment is. I would urge you to read it by clicking on the link https://scroll.in/pulse/844442/children-are-dying-of-cancer-for-lack-of-money-even-those-that-get-free-medical-treatment
Recently a journalist Ankur Paliwal contacted me as he wanted to highlight this issue. He met others as well and has published a nice piece which tries to bring together all viewpoints and highlights very well, the social problem that abandonment of treatment is. I would urge you to read it by clicking on the link https://scroll.in/pulse/844442/children-are-dying-of-cancer-for-lack-of-money-even-those-that-get-free-medical-treatment
Sunday, 30 April 2017
Best Childhood Cancer Blogs on the Planet
I have been blogging for many years now. I would like to do it more frequently and put better content, but then there are always competing priorities. This week I was surprised to receive this email in my inbox
Hi Childhood Cancer India Team,
My name is ____________. I'm Founder of Feedspot.
My name is ____________. I'm Founder of Feedspot.
I would like to personally congratulate you as your blog Childhood Cancer India has been selected by our panelist as one of the Top 75 Childhood Cancer Blogs on the web.
http://blog.feedspot.com/childhood_cancer_blogs/

I personally give you a high-five and want to thank you for your contribution to this world. This is the most comprehensive list of Top 75 Childhood Cancer Blogs on the internet and I’m honored to have you as part of this!
Also, you have the honor of displaying the badge on your blog.

Recognition like this was completely unexpected but also welcome. More importantly I want to thank Feedspot for compiling a list of 75 childhood cancer blogs. Such information will be enormously useful to many people
Wednesday, 15 February 2017
Happy International Childhood Cancer Day
Today is International Childhood Cancer Day. It is an opportunity to focus the attention of the public, the health professionals and the government on this cause. International and national efforts are underway and you can read more about them at the following links
Below is a very useful infographic prepared for this occasion.



Wednesday, 26 October 2016
Prevent Toddlers from Cancer! - Max Healthcare
Prevent Toddlers from Cancer! - Max Healthcare: Prevent Toddlers from Cancer!
Saturday, 20 August 2016
We Are One!
Earlier this year, Childhood Cancer International, the largest patient support organization for childhood cancer with 181 member organizations in 90 countries, teamed up with Christophe Beck, famous for his creation of the soundtrack to Disney’s smash hit Frozen, and his 12-year-old daughter to record a new song, “We Are One,” written just for International Childhood Cancer Day (February 15th). While the verses are sung by up-and-coming musical talents including Sophie Beck, Alexa Curtis (winner of The Voice Kids Australia 2014), Livvy Stubenrauch (the voice of Anna in Disney’s Frozen), and Robbie Firmin (Britain’s Got Talent), the chorus is a global choir of all the children who participated in this amazing event! The creative responses have been overwhelming with More than 900,000 children and teens recorded their voices singing the chorus to the song, creating dances, lip-syncing videos, and even creating some amazing covers! Here is the official video below. Enjoy!
Subscribe to:
Posts (Atom)